Clinical Practice/Forensic
ORIENTATION AND OUTLINE
This unit presents basic information regarding forensic testimony about qEEG findings and how they may be useful in a courtroom setting. Although this information is drawn from American federal and state jurisdictions, the principles apply worldwide.
Please click on the podcast icon below to hear a lecture over this unit.

In addition to forensic terminology and the application of standards for testimony such as Frye and Daubert, this section presents important clinical issues for qEEG providers. These include review of conditions that may be suitable for qEEG evaluation, clarifying and determining the appropriateness of the referral for qEEG, choice of reference databases, limits of interpretation, clinical versus statistical probability, necessity of reviewing client history and existing reports, and consideration of how qEEG findings correlate or not with other clinical evidence. Graphic © Gorodenkoff/Shutterstock.com.

IQCB Blueprint Coverage
This unit covers IX. Clinical Practice/Forensic (4 Hours)

This unit covers:
A. Knowledge regarding the limits of interpreting the QEEG regarding the choice of reference databases and recognizing statistical probability versus clinical probability
B. Recognizing the difference in deposition as a "fact/treating" witness vs. an "expert" witness
C. Understanding the Daubert vs. Frye standards and their application to the QEEG
D. Emphasis of correlating the QEEG with other clinical diagnostic evidence
E. The appropriateness of a QEEG referral
F. Patient conditions related to QEEG evaluation
G. History and prior clinical and laboratory reports review
A. The Limits of Interpreting the QEEG and the Issue of Probability
The choice of reference database can significantly impact the interpretation of qEEG data, influencing connectivity patterns and network properties. Each type of normative database poses its own special requirements and details, which can affect the interpretation of qEEG data (Thatcher & Lubar, 2023).
What should one consider when choosing a normative database? These facts are also reviewed in qEEG Tutor’s section on normative databases. In addition to those factors, it is important to consider the referral question and client-specific details when selecting a normative database. For example, when assessing a client with autism spectrum disorder, where connectivity is often an issue, it is important to select a normative database that includes measures of coherence. When assessing clients who have posttraumatic stress disorder where the default mode network may show dysrhythmias, it is important to select a database that images that network, if not the structures involved.
Critical issues include the concept of normalcy, norming of qEEG features, and validation of clinical findings, which are essential for accurate interpretation. Technical aspects such as recording methods, filter use, frequency resolution, and statistical testing are crucial for the construction and use of these databases (Johnstone et al., 2003).
The choice of reference database and electrode significantly impacts qEEG interpretation, affecting both connectivity patterns and network properties. Consistent reference schemes and careful consideration of normative database features are essential for reliable and accurate qEEG evaluations.
All tests have limits, as does qEEG. Further, the various normative databases used for qEEG each have particular strengths and limitations that can affect the interpretation of qEEG data (Thatcher & Lubar, 2023). Understanding these strengths and limitations depends on formulating a clear referral question. With a clear referral question, the qEEG provider can then decide whether qEEG methods are generally appropriate and whether a given normative database suits the specific needs of addressing the referral question. Suppose qEEG is a valid method for assessing the type of client who has been referred. In that case, the practitioner then essentially asks, “Which of the available normative databases is best suited to the details of the referral question given their respective strengths and limitations?”
Understanding the limitations of interpreting qEEG findings and the questions it can answer is crucial. Livint Popa and coauthors (2020) offer a comprehensive review of diagnoses where qEEG findings can be integrated with data from other sources. For instance, qEEG findings can be instrumental in diagnosing conditions like epilepsy, stroke, dementia, traumatic brain injury, and mental health disorders such as ADHD, autism spectrum disorder, anxiety, and depression. Koberda (2021) further explores the benefits of qEEG in the assessment of dementia and traumatic brain injury. The use of qEEG in a forensic setting is detailed below.
Other uses of qEEG are reviewed in the section of qEEG Tutor’s normative databases section. However, qEEG is limited in that it cannot serve as the sole type of information on which to base an assessment, diagnosis, treatment formulation, or outcome evaluation. Rather, qEEG findings should be integrated with information from other sources. Doing so helps to guard against assigning significantly large importance to isolated findings that are statistically significant without meaningfully correlated findings of clinical significance.
Although the qEEG's strength is its temporal resolution, its spatial resolution is weak, for example, compared to MRI. Further, there are CNS structures, particularly subcortical structures, that qEEG cannot image. Other strengths of qEEG are its ability to image connectivity, including effective connectivity, in many CNS networks and its ability to demonstrate activity outside well-defined norms with respect to multiple metrics.
Statistical Versus Clinical Probability
A common dilemma for clinicians who rely on scientifically-informed findings is understanding the difference between the statistical significance of a finding and its clinical significance. One does not imply the other, and both must be considered when making reports or other statements and clinical decisions. Statistical and clinical significance can also be reframed as statistical and clinical probability.Statistical probability is fundamentally concerned with the likelihood of an event occurring based on mathematical principles and data analysis. It is often used to determine the significance of research findings through hypothesis testing and the calculation of p-values (Stratton et al., 2018).
Statistical probability involves hypothesis testing, where a null hypothesis (no effect) is compared against an alternative hypothesis (effect present). The p-value indicates the probability that the observed data would occur if the null hypothesis were true. A smaller p-value (typically ≤ 0.05) suggests that the observed effect is statistically significant, meaning it is unlikely to have occurred by chance.
Another key aspect of statistical probability is the use of confidence intervals, which provide a range within which the true value of an effect is likely to lie. A 95% confidence interval, for example, means there is a 95% probability that the true effect size falls within the specified range. This helps in understanding the precision and reliability of the estimated effect.
Clinical probability, on the other hand, is more focused on the practical implications of research findings in a healthcare setting. It considers the real-world impact of an intervention or treatment on patient outcomes.
The clinical approach is often deterministic and causal, emphasizing diagnosis and treatment over mere prediction. It is less concerned with the statistical significance of findings and more with their practical relevance and applicability in clinical practice (Einhorn et al., 1986).
Clinical probability assesses the magnitude and importance of an effect in a real-world context. An effect that is statistically significant may not always be clinically significant. For instance, a small effect size that is statistically significant might not have meaningful implications for patient care. Conversely, a clinically significant finding may not always achieve statistical significance but could still be crucial for treatment decisions (Stratton et al., 2018).
B. Forensic Medicine
Actions of a legal nature involve applications of laws to adjudicate differences, where the term “law” is a term derived from “lex,” the Latin word for law. These legal actions are “adversarial” in the sense that they “involve two or more interested parties who must reach a resolution of a common concern or disagreement from potentially antagonistic positions” (Sweet, Kaufman, Ecklund-Johnson, & Malina, 2018, p. 857). Such legal actions are sometimes called forensic, a word based on the Latin word “forum,” which was a place for public debate in Rome.
Legal disputes to settle differences often require expert testimony, which in some cases is testimony about health or medical conditions. Medical testimony does not necessarily require a physician, but does require testimony by experts who are accepted or qualified by a judge to provide an opinion within their scope of expertise. Similarly, the terms “medical” and “medicine” are defined as involving not only physicians but also the many disciplines that provide assessment and treatment for a range of health conditions.
Neuroscience Evidence
Aono, Yaffe, and Kober (2019) review the history of neuroscience in court and define neuroscientific evidence as any information about the brain. Neuroscientific evidence has been used in court since the early 20th century, with its use in criminal cases increasing in the 21st century.As Jones (2013) summarized, there are seven main categories of forensic neuroscientific evidence. These are: “buttressing (the use of neuroscience as supporting evidence); detecting (the use of neuroscience to gain otherwise elusive insights, such as the extent of brain injuries); sorting (the use of neuroscience to categorize people into legal classifications, such as sane versus in insane); challenging (the use of neuroscience to challenge an institutionalized assumption); intervening (the use of neuroscience to create and recommend interventions); explaining (the use of neuroscience to shed light on uncontested, yet not well understood phenomenon); and predicting (the use of neuroscience to help make predictions about people’s future behavior)” (Aono et al. 2019, p. 4).
Neuroscientific evidence can be used like any other evidence to establish or dispute a claim. For instance, neuroscientific evidence could support or challenge the credibility of an expert witness, increase or decrease the likelihood of a diagnosis, support testimony about a defendant’s state of mind, show the severity of injury, help the trier of fact understand some other evidence, etc. An overview of the discipline of so-called neurolaw is given by Jones and Shen (2011).
Effects of Neuroscience Evidence on Legal Decisionmaking
Research to date suggests that neuroscientific evidence has some mitigating effects, for example, in cases of the death penalty (Aona et al., 2019). While neuroscience testimony may affect the verdict, the finding of insanity, and sentencing, the type of mental disorder (i.e., schizophrenia vs. psychopathy) and perceived dangerous may also moderate this effect. However, brain images per se have little persuasive effect despite their allure in nonlegal contexts (Aona et al., 2019, p. 17).As summarized by Aono et al. (2019), experimental comparisons of expert testimony to expert testimony plus neuroimages show no significant mitigating effect among mock jurors with respect to their verdict of sentence severity. Although initial studies suggested that neuroimages were uniquely persuasive (Aono et al., 2019, p. 17), such effects were not replicated.
Aono et al. (2019) summarize results from the studies they reviewed, writing that the neuroscientific evidence reduced death penalty sentences across studies under most conditions and increased not guilty by reason of insanity (NGRI) verdicts, but did not increase non-NGRI not guilty verdicts or influence length of prison sentences.
Aono et al. (2019) suggest that neuroscientific evidence might be mitigating because jurors see such evidence as more satisfying and impactful, consistent with research supporting the idea that jurors prefer reductive evidence across the neurosciences (p. 18). This remains an open question.
An additional hypothesis supported by some studies suggests that neuroscientific evidence may mitigate jurors' perception that the defendant has less-than-normal self-control. According to Aono et al. (2019, p.19), the mechanism by which neuroscience evidence has mitigating effects is likely juror perception and other cognitive factors. However, no study has addressed this hypothesis directly.
Other gaps in the studies reviewed by Aono et al. (2019) are the investigation of effects due to race, sex, and cases that do not involve murder or assault (e.g., property and drug crimes). Citing Greene and Cohen (2004), Aono et al. (2019) wrote that it is “ultimately possible that the greatest contribution of neuroscience to criminal justice will be its influence on how people think about free will, responsibility, and treatability in the context of criminal behavior, rather than to influence the legal decisions they make” (p. 19).
Neuroimaging in Court
Miller and Lindberg (2017) offer a recent review of various neuroimaging methods, how they may be helpful in forensic settings, and cautions to bear in mind. As summarized by Miller and Lindbergh (2017), Meixner (2015) writes that the “basic function of the law is to regulate behavior, and neuroimaging methods are among the most powerful, robust, and objective tools available to shed light on the biological mechanisms underlying behavior” (p. 129). Miller and Lingbergh (2017) focus their review of structural and functional neuroimaging methods in court with respect to brain damage and mild traumatic brain injury (mTBI), discussing EEG techniques only in the category of functional neuroimaging. Their review provides an excellent overview of each method, its strengths and weaknesses, and its relevance for forensic testimony. These authors note that functional neuroimaging, with its emphasis on physiological and metabolic activity, complements methods that assess structural integrity. As Miller and Lindbergh note, functional neuroimaging can be especially important because brain injury and recovery are dynamic, with sequelae that unfold over time across several levels of analysis (e.g., individual neurons, networks, cognition, emotion, and behavior). That is, qEEG findings may help track an injury's evolution and recovery.As discussed by Miller and Lindbergh (2017), qEEG measures provide important information about brain regions' connectivity and the timing and direction of neuronal activity. Compared to other methods, qEEG data, like MEG and ERP data, have excellent time resolution but limited spatial resolution and depth of signal detection. Furthermore, qEEG methods, according to Miller and Lindbergh, have limited specificity (i.e., with the pattern of qEEG findings being limited to only a specific condition) and reliability (in the sense of producing findings replicated across scientific studies). Nevertheless, EEG data have the potential to supplement the diagnosis and treatment of many disorders (e.g., mood disorders, learning disabilities, schizophrenia, chronic pain, and Alzheimer's disease; Leiser, Dunlop, Bowlby, & Devilbiss, 2011).
EEG methods are also prominent in the monitoring of epileptic conditions (Maganti & Rutecki, 2013), with Gutmann (2007) describing its application in the famous case of Jack Ruby, who shot and killed President John F. Kennedy’s assassin, Lee Harvey Oswald.
Miller and Lindbergh (2017) indicate that qEEG can be especially relevant to cases of TBI because of its superior temporal resolution, but also, however, that EEG is not routinely used following traumatic brain damage. Studies investigating EEG have shown somewhat inconsistent findings, though generalized or focal slow wave activity and attenuated posterior alpha activity have been reported within several hours post-injury (Nuwer, Hovda, Schrader, & Vespa, 2005). Different investigators have found different EEG abnormalities (e.g., generalized bursting) or the absence of abnormality entirely (Arciniegas, 2011). Different severities of TBI may account for such discrepancies, with excess slow-wave activity being more likely among severely injured patients (Thatcher, North, Curtin, Walker, Biver, Gomez, & Salazar, 2011).
EEG measured within 24 hours of TBI has some predictive value, showing a correlation between abnormality and outcome 23 years later when factored in with posttraumatic amnesia (Hessen & Nestvold, 2009). Persisting EEG abnormality is predicted by the degree of abnormality in the acute phase of injury (Rapp, Keyser, Albano, Hernandez, Gibson, et al., 2015). Changes in the ratio of local to distant connectivity (i.e., reduced Theta clustering) after mTBI has been found (Tsirka, Simos, Vakis, Kanatsouli, Vourkas, et al., 2011) and interpreted as showing neural disorganization. Despite the typical normalization of EEG changes within a few months post mTBI, some findings, such as diffuse intermixed slowing, may continue in some cases. However, this may be due to confounds such as medication (Arciniegas, 2011).
Forensic Value of qEEG Findings
Presentation of qEEG results in forensic settings helps to inform the court about a litigant or claimant’s brain health and how that might be related to the person’s behavior, cognition, or emotional functioning so that the trier of fact, whether a judge or jury, can better make a just legal decision such as a verdict or sentence in the case. Because of its quantitative nature, use of normative values, and basis in brain science, qEEG findings can serve as a credible source of information in legal proceedings.qEEG findings may be of interest in forensic cases for several reasons. Because the brain has an extremely significant role to play in behavior, the understanding that qEEG provides about the brain’s integrity can help the trier of fact in formal or informal proceedings make well-informed decisions about the nature and degree of injury, its effects on the brain, as well as about disability, prognosis, and culpability so that the trier of fact can reach a just adjudication. The quantitative nature of qEEG findings imparts them with an objective character, particularly because findings are compared to norms. The scientific foundation of qEEG methods furthermore leads to a discussion that is helpful in forensic hearings insofar as it embodies consideration of hypotheses and their alternatives regarding the subject’s diagnosis or condition, levels of certainty, an acknowledgment that studies have limitations, willingness to address potential criticisms, and demonstration of reasoning that logically traces propositions from the general, nomothetic scientific literature to the specific idiographic individual case in the context in which it occurs. These latter qualities parallel the types of thinking that the trier of fact must employ to reach their decision in a legal case.
qEEG findings can be likened to findings from any other medical tests, particularly other biological tests of brain structure and function (cf. CT, MRI, fMRI) (Miller & Lindbergh, 2017). They are meaningless unless interpreted in the context of personal history, other tests, normative values, and the network of research on which brain science is based. The degree to which such interpretation can be usefully made in any legal case depends on its relevance, scientific reliability and validity of the method, the type of findings that bear on the case, and the expertise of the professional who conducts the interpretation. At the least, interpretation of qEEG results should be made by a professional who is thoroughly knowledgeable about the EEG and how it is measured, scientific and statistical methods, and applying qEEG findings to cases resembling the one at issue in the legal matter that presents itself. Further, an interpretation of qEEG findings should be made by someone who thoroughly understands brain-behavior relationships and health at levels of impairment, disability, and handicap (Carter, 2023; Thatcher, 2010).
qEEG findings provide information about the possible location and type of brain dysfunction a litigant may present (defendant, plaintiff, claimant). Such findings may implicate disruption of central nervous system structures and their interactions. However, mere disruption of function (i.e., an impairment) may be irrelevant unless the functions involved and related abilities are pertinent to the mental condition or behavior (i.e., action, ability/disability, or handicap/participation) at issue in the legal proceedings. The ecological validity of qEEG findings is at stake and is best supported by logical reasoning and empirical links between CNS function and real-world behavior. For example, a qEEG finding of significantly abnormal cortical activity in the left frontotemporal region (an impairment) is only imperfectly correlated with language function (an ability), let alone use of language at the sales desk of an auto parts store (participation in a vocational role). Therefore, qEEG findings may be only one thread in the entire fabric of evidence weighed by the trier of fact when they decide that the totality of evidence reaches the threshold of the civil or legal burden of proof (i.e., the balance of probabilities or beyond a reasonable doubt, respectively).
qEEG findings carry more weight when they are consistent with other case-related data. qEEG findings may be considered in terms of their consistency with the claimed etiology of a brain injury, the severity of damage documented by other means, and behavioral observations (Greiffenstein & Kaufmann, 2018). Consistency with nomothetic (general scientific) factors is also important to consider. For example, do the qEEG findings conform to a nomothetic dose-response curve where more severe damage (dose) has reliably been found with scientific methods to produce more severe qEEG findings (response)? Or, do qEEG findings of dysfunction in the orbitofrontal region conform to a scientifically reliable association between damage to that region and disinhibited behavior?
qEEG findings are one piece of data that can help the trier of fact appreciate that an individual’s thinking, emotion, or behavior has been or is currently affected by brain dysfunction. In civil and criminal matters, qEEG results may be one of several objective data points that converge to help the trier of fact when considering a legal decision. If the question is one of diagnosis and its effects, qEEG findings alone will not answer it. However, a qEEG finding that shows dysfunction of particular regions of interest or networks may converge with other findings related to cognition, emotional function, and behavior or, in fact, with a diagnosis. For example, a finding of disinhibition in the contexts of results from neuropsychological and other tests, physical examination, and behavioral observations may be further strengthened as a consideration for the trier of fact when qEEG results show dysfunction of the orbitofrontal cortex (OFC), with the additional provision of scientific knowledge to the trier of fact that the OFC is involved in inhibitory control.
qEEG findings may be of value for the trier of fact insofar as they help to stage the severity of brain dysfunction (cf. Greiffenstein & Kaufmann, 2018). This may be the case even with mild traumatic brain injury (mTBI), a condition that presents many thorny conundrums. For example, many clinical neuropsychologists assert that late post-concussive symptoms (LPCS) following mTBI (e.g., symptoms that begin following concussion and continue for a year or longer) are most likely not due to any persistent neurobiological dysfunction or structural damage but instead relate to a complex of psychological, social, and environmental factors that perpetuate early symptoms that involve brain injury or worsen predisposing conditions.
The genuine, though transitory, disruption of neurochemical and network connectivity processes seen in mTBI may, however, be an immediate effect of the precipitating concussive event along with its associated physical and psychological trauma and consequent disruption of functional activities. Objective qEEG findings, either soon after injury or in the several months following, may demonstrate changes in connectivity measures (Thatcher et al., 1989) and, in this way, help the trier of fact to consider the possibility that biological changes related to injury may have been significantly involved in the initiation of cognitive, emotional, and behavioral changes. An immediate brain-related datum (i.e., qEEG findings) that is consistent with the severity of a precipitating injury may then be understood as showing changes in the brain that contribute to the initiation of injury-related impairment and disability, which in turn are maintained by perpetuating factors of a psychological and socially-mediated type that act on a person who may have predisposing vulnerabilities. Nevertheless, recent research shows that mTBI can produce lasting changes to the brain that may also be involved in persistent symptoms (see below).
There is typically a dose-response relationship following TBI, with injury severity positively correlated with the severity of cognitive impairment. Nonetheless, it is wise to heed Greiffenstein and Kaufmann's (2018, p. 902) advice to "always be open to new and objective case-specific information that may 'trump' base rates and provide compelling evidence" of long-term symptoms that are attributable to mTBI, that is directly to trauma-related changes to brain structure and/or function that may be objectively identified only with specialized tests (Dean & Sterr, 2013).
Whereas many clinical neuropsychologists assert that there are virtually no measurable cognitive differences several months post-injury between groups of mTBI and normal subjects, such findings may not account for the increased effort required by mTBI subjects to achieve normal performance levels. As attributed to Carl Sagan, "Absence of evidence [in this case, of biological or cognitive differences between mTBI and normal subjects one-year post-injury] is not evidence of absence." To that point, and that of Greiffenstein and Kaufmann's (2018, p. 902) advice, there is some accumulating research that shows evidence of cellular, perfusion, and both functional and structural connectivity changes long after mTBI among some subjects, which may have implications for emotional function, independent activities of daily living, socialization, and work performance (Chan et al. et al., 2015; Dall'Acqua et al. et al., 2017; Kan et al., 2012; Lemme et al. et al., 2021; Papadaki et al. et al., 2021).
The trier of fact may find the objective qEEG findings probative and as contributing to the body of evidence they use to judge whether the event at issue and its injuries have led to persisting loss of function that merits compensation. Nevertheless, in cases of mTBI, neurotoxicity, or other maladies, it is important to avoid reasoning that an exposure or trauma of a magnitude that does not normally lead to persistent, significant brain injury, plus nonspecific subjective complaints, is sufficient proof of chronic changes to the brain that can only be found with qEEG methods of assessing brain function. Knowing the relevant science and avoiding reasoning beyond one’s data is important.
The greatest value of neuroimaging and qEEG in court is when it is integrated with data from other sources. Miller and Lindbergh (2017) suggest that several studies have found that neuroimaging improves the accuracy of specific conclusions about brain injury and the meaningful consequences thereof, and that complementary methods such as qEEG and fMRI are prime candidates for combination (Miller & Lindbergh, 2018, p. 134; Mayer, Bellgowan, & Hanlon, 2015).
Legal Settings for Testimony
The settings in which expert testimony occurs may be formal, in which case they may occur in a courtroom and involve criminal actions (insanity defense, mitigation of culpability, death penalty sentencing), civil (personal injury, medical malpractice), probate-related, or involving family law such as custody and divorce. On the other hand, informal settings address matters such as administrative actions (e.g., disability determination, fitness for duty, educational entitlement, and alternate dispute resolution). These different settings and types of actions (administrative, civil, criminal) often differ in their level of burdens of proof, rules of evidence, and trier of fact. Instead of providing qEEG services to a patient who wants health care assessment and treatment, qEEG findings in forensic contexts are outside usual clinical care and require the expert witness to be knowledgeable about the specific rules that apply to the type of action for which testimony is provided (Sweet et al., 2018).The specialty knowledge regarding qEEG findings is given to the “trier of fact” (i.e., a judge, jury, or panel) so that they can decide the case of a litigant (defendant or plaintiff in formal court proceedings) or a claimant (or applicant in less-formal proceedings). Regardless of the setting, testimony about qEEG should help educate the trier of fact to make the legal decision that is their sole responsibility.
Administrative settings are a hybrid between civil court and adjudication by government agencies, as in the case of worker’s compensation claims. A magistrate holds a hearing in which the magistrate and other hearing officers determine the facts using somewhat relaxed rules of evidence. As in license revocation, a governmental agency may be a party to a dispute. The burden of proof is usually the preponderance of evidence.
Probate settings probe into facts related to the creation and execution of wills.
Civil settings adjudicate issues of liability and damages, with the preponderance of evidence being the standard of proof. Issues of fact that the jury may decide are whether there is a neurological injury and whether such injury resulted in deficits.
Civil and administrative legal actions are tort suits. Civil torts (e.g., car collisions, medical malpractice) address matters of duty, foreseeability, negligence, causation, and damages. Administrative torts involve seeking compensation of a legal benefit where causation is not an issue (e.g., educational accommodations).
Criminal settings involve issues that may infringe liberty, for example, when a defendant is in jeopardy of incarceration or execution following a conviction of guilt. In criminal settings, the burden of proof is much higher than in civil cases, and conviction rests on a finding that culpability is greater than a reasonable doubt.
Levels of Legal Authority
The structure of the law involves issues of authority, where greater authority is more favorable to one party or another in a legal action. As outlined by Greiffenstein and Kaufmann (2018), there are several types of authority, and these include primary, secondary, binding, and persuasive. Primary authority (e.g., case law, regulations) derives from the government directly and requires court interpretation. Secondary authority includes opinions and commentaries set out, for example, by an attorney general or a governmental agency. Only laws with primary authority can be binding or controlling in their application, depending on jurisdiction and the specific facts in a case. If an earlier finding with primary authority is binding in a current case, then the current case must base its decision on the earlier finding. On the other hand, other laws and findings may not be binding but only persuasive based on their use of reasoning, factual similarities, or judicial reputation.Court opinions may be either published or unpublished. Published decisions, such as the U.S. Supreme Court’s decision in Daubert v. Merrell Dow Parm. Inc. (1993) have broad scope that judges must follow in future actions. Unpublished decisions involve rulings that apply with limited scope to a particular case.
In the U.S., a hierarchy of authority in the court system prevails in criminal matters. Graphic from lumenlearning.com/suny-osamgovernment.
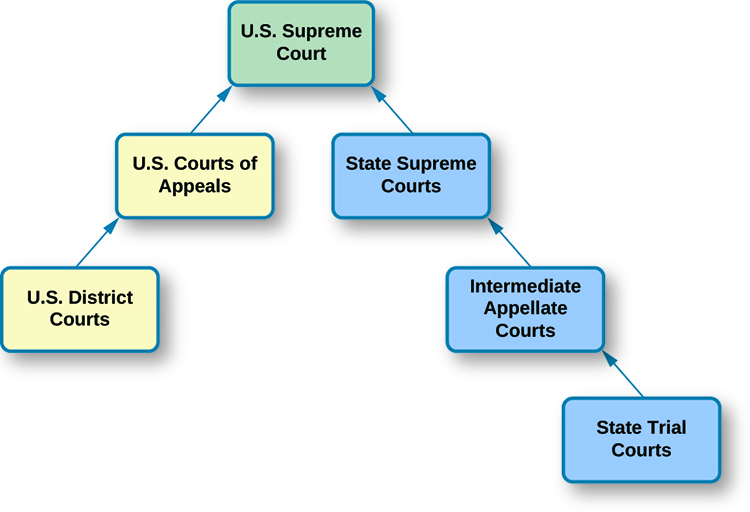
Federal cases are tried first in U.S. District Courts. Convictions can be appealed to a U.S. Court of Appeal, also known as a circuit or appellate court. Subsequently, the case may be appealed to the U.S. Supreme Court.
State cases are first tried in state trial courts and may be appealed to intermediate state appellate courts before being appealed to the state Supreme Court. Cases may also then be appealed to the U.S. Supreme Court.
Trier of Fact
In any legal setting, the final judgment or decision is made by the trier of fact, who may be a judge, panel of adjudicators, or a jury. Only the trier of fact, whether a jury or possibly a judge, can decide ultimate legal questions, for instance, of causation (e.g., this gunshot wound caused this plaintiff’s brain damage). qEEG testimony can provide a penultimate opinion just short of the ultimate question by saying, for example, that the qEEG findings are consistent with a penetrating brain injury of the type found in the plaintiff or with ADHD in an administrative case involving access to benefits or accommodations.Burden of Proof
Civil and criminal trials have different burdens of proof, that is, the level of certainty with which the trier of fact reaches their verdict.In civil litigation, the lowest standard of proof is used: balance of probabilities or preponderance of the evidence. This means that the evidence proves the point at issue with over 50% confidence. In criminal litigation, on the other hand, a higher burden of proof is required, being beyond a reasonable doubt. This is often interpreted as certainty of about 90%. Clear and convincing proof is an intermediary standard of certainty of about 75%.
In criminal trials, the defendant enters with a presumption of innocence, and the state or federal authority that brings charges carries the burden of proof to persuade the trier of fact beyond a reasonable doubt that the defendant committed the crime charged. An exception is the claim of insanity when the defendant has the burden of proving to the trier of fact that s/he was insane at the time of the crime. Many jurisdictions require insanity to meet only the “clear and convincing standard.” In civil cases, the applicant or plaintiff must prove their case against the defendant.
Capacity and Competence
Insanity is a legal term that according the Legal Information Institute of Cornell Law School:refers to a mental illness or disease that makes it impossible for a defendant to know they were committing a crime or to understand that their actions are wrong. A defendant found to be criminally insane can assert an insanity defense. Insanity functions as a failure of proof defense where the defendant admits to having committed the wrongful act, but claims … they are not culpable because of their mental defect prevented them from establishing the required mental state.
Tests to determine if a defendant is criminally insane vary from state to state. For instance, any jurisdiction that follows the Model Penal Code (MPC) rule looks to see if the defendant lacked both substantial capacity to appreciate the wrongness of their actions and substantial capacity to conform their actions to the law. Jurisdictions that follow common law tests are primarily split between the M'Naghten Rule and the irresistible impulse test. Under the former, a party is criminally insane if they lacked the capacity to know they were committing a crime due to a mental defect. Under the latter, a defendant is criminally insane if they lacked total capacity to know they were committing a crime due to a mental defect. Under the latter, a defendant is criminally insane if they lacked total capacity to conform with the law.
Issues of capacity and competency can be involved in civil matters. Mental capacity refers to the functional ability to carry out a specific activity (e.g., medical decision-making, making a contract, communicating with counsel, etc.). In contrast to an expert witness’s testimony about capacity, competence (e.g., activities noted parenthetically above) is determined by a judge or legal body, relying on evidence that a medical condition is causative. In competency hearings, capacity is only one consideration. In criminal trials as well, competence may also be an issue.
According to Sweet et al. (2018), types of competencies relate to:
• waiving Miranda rights.
• waiving the right to counsel.
• standing trial.
• understanding advisements of rights and validity of confessions.
• entering a plea.
• criminal responsibility.
• the advisability of defendant testifying.
• sentencing.
• being executed.
Federal Rules of Evidence
The trier of fact in a legal proceeding uses evidence and reasoning to reach a verdict. One source of evidence is from expert witnesses. A judge uses rules of evidence to qualify an expert witness to present particular pieces of evidence and to admit evidence to a court.Depending on its relevance, evidence may be prejudicial or probative. Prejudicial evidence is not admissible because of its likelihood of producing strong emotional reactions among jurors that may sway their reasoning and decision unfairly. Probative evidence is admissible and likely to be directly relevant to juror decisions. If evidence is both probative and prejudicial, a judge may weigh one against the other to judge the merit of admitting it as evidence.
The testimony or opinion provided by an expert must be probative/relevant and not prejudicial. Or, the testimony must at least be more probative than prejudicial on balance.
Greiffenstein and Kaufmann (2018) review Federal Rules of Evidence (FRE) that are relevant for neuroscientific testimony, for example, by neuropsychologists (Federal Rules of Evidence, 1975). They are likely to interest those presenting qEEG findings in court. These rules for the admissibility of evidence and qualifying expert witnesses to testify are substantially in force in most US states.
As Greiffenstein and Kaufmann (2018) summarized, Rule 401 defines evidence as relevant when it makes “the existence of any fact that is of consequence to the determination of the action more probably or less probable than it would be without the evidence.” Rule 402 further specifies that evidence not be overly prejudicial.
Two types of witnesses are mentioned in the FRE. Lay (fact) witnesses (FRE 701) present evidence they have acquired only by their senses. For example, lay witnesses include treating health professionals or bystanders who saw an event occur. A second type of witness is an expert witness (FRE 702) who gives an opinion about the meaning of evidence. The expert is qualified to testify by their knowledge, skill, experience, training, or education. A qualified witness whom a judge has qualified to testify may provide an opinion if the testimony is based on sufficient facts or data. Testimony must be the product of reliable principles and methods, and the expert must reliably apply the principles and methods to the facts of the case. In the case of qEEG testimony, the expert helps the trier of fact understand the evidence and what the findings mean. This may involve presenting scientific information about the brain-behavior relationship, development and use of qEEG methods, electroencephalographic activity and its relationship to brain dysfunction, the relationship of any qEEG abnormality to potential brain or behavioral dysfunction, and the relationship of qEEG findings to behavior.
FRE 703 is a so-called hearsay rule that allows the qEEG expert to provide an opinion on non-qEEG data so long as it is “reasonably relied upon” by experts in a particular field. This allows opinions regarding plaintiff/defendant/applicant history and reports produced by other experts to be integrated with the qEEG findings.
FRE 704 sets boundaries for expert opinion and addresses the issue of penultimate and ultimate opinions. The first part of this rule allows experts to give opinions similar to the legal decisions of the trier of fact, and the second part specifies that the expert must not give ultimate opinions regarding a defendant’s state of mind. For example, an expert may say that qEEG findings are likely to have been caused by an accident like the one at issue, with cognitive or behavioral disturbances likely to be of a particular type. Still, they may not give an opinion about how those findings or disturbances bear on criminal culpability (i.e., the ultimate decision, which is the responsibility of the trier of fact). An example of an appropriate penultimate opinion might be that “the defendant was likely suffering from a significant brain disturbance consistent with a traumatic brain injury, and which may have been associated with significant cognitive and behavioral disturbances around the time of the crime.”
C. Daubert vs. Frye Standards
U.S. Supreme Court Decisions on Admissibility
Standards of admissibility of evidence were developed to reduce the risk that legal matters would be vulnerable to pseudoscientific evidence that is based on methods that cannot be replicated (i.e., are unreliable for producing similar results with similar methods at different times and in different places).Sweet et al. (2018, p. 866) state that “it is important to recognize that decisions involving evidentiary standards are case-specific and are influenced by the individual expert, the procedures he or she uses, and the underlying scientific evidence in a particular case. Thus, it is quite possible that a particular expert’s testimony might be accepted in one instance and denied in another, depending on whether his or her assertions in each specific case are judged to have a valid scientific base.” It is important to avoid speculative opinions that stray beyond what the data support.
Frye Standard for Admissibility of Evidence
For most of the 20th century, the Frye standard (Frye v. United States, 1923) gave requirements for the admissibility of evidence. This standard stated that experts can give evidence that must be “generally accepted” in their field of scientific practice. This criterion attempts to limit speculation and “junk science.” However, the general acceptance rule is problematic because of difficulties determining which scientific community applies and the degree of acceptance based on a small number of experts testifying in a particular case. It may also bar recent advances that are valid but not known generally or permit admission of invalid techniques because most scientists and practitioners still believe them (Greiffenstein & Kaufmann, 2018; Melton, 1997).
Daubert Standard for Admissibility of Evidence
Daubert v. Merrell Dow Pharms., Inc (1993) and subsequent cases include the Frye requirement for evidence to meet the standard of “general acceptance,” and assert that the gatekeeping function belongs to the judge, who considers whether the expert’s methodology was subjected to peer review, is testable (falsifiable), and has a known error rate.
As summarized by Sweet et al. (2018), other factors the judge should consider when evaluating whether testimony is admissible are whether:
• the expert will testify about matters related to their own research or whether their opinions are only for the purposes of testimony;
• the expert extrapolates unreasonably from an accepted premise to an unfounded conclusion;
• the expert is as careful in testimony as in regular professional work outside the courtroom and
• the field of expertise reaches reliable results for the expert's opinions.
Daubert evidentiary standards are met when tests are standardized, reliable, valid, norm-referenced, and have technical manuals or presentations in peer-reviewed publications. (Sweet et al., 2018, p. 859).
qEEG methods for describing disturbances of brain structure and function may sometimes have difficulty reaching the Frye criterion, particularly if findings are used to provide testimony beyond what existing science can sustain. However, if provided prudently and with a solid scientific foundation that the testimony references, qEEG findings may achieve the threshold of being viewed as generally accepted in a given case, despite the now-outdated Nuwer (1997) report. Although Greiffenstein and Kaufmann (2018) write that qEEG has consistently been ruled inadmissible as the only proof of any physical or psychological diagnosis (cf. SPECT), it may, as SPECT has been, be admissible as a supplement to the findings of other tests, that is, as showing qEEG findings “consistent with” a diagnosis or impairment determined by other means.
In 1993, the U. S. Supreme Court ruling in Daubert v. Merrell Dow Pharm., Inc. updated the rules of evidence. Although most states use the Daubert standards, a few continue using Frye.
Different authors give somewhat different listings of standards of admissibility under Daubert. Wikipedia describes Daubert with the following guidelines for admitting scientific expert testimony (Wikipedia, accessed 16 August 2023):
1. Judge is gatekeeper: Under FRE Rule 702, the task of "gatekeeping," or assuring that scientific expert testimony truly proceeds from "scientific knowledge," rests on the trial judge.
2. Relevance and reliability: The trial judge must ensure that the expert's testimony is "relevant to the task at hand" and rests "on a reliable foundation." Daubert v. Merrell Dow Pharms., Inc., 509 U.S. 579, 584-587. Concerns about expert testimony cannot be simply referred to the jury as a question of weight. Furthermore, the admissibility of expert testimony is governed by Rule 104(a), not Rule 104(b); thus, the judge must find it more likely than not that the expert's methods are reliable and reliably applied to the facts at hand.
3. Scientific knowledge = scientific method/methodology: A conclusion will qualify as scientific knowledge if the proponent can demonstrate that it is the product of sound "scientific methodology" derived from the scientific method.
4. Illustrative factors: The court defined "scientific methodology" as the process of formulating hypotheses and then conducting experiments to prove or falsify the hypothesis and provided a set of illustrative factors (i.e., not a "test") in determining whether these criteria are met: 1. Whether the theory or technique employed by the expert is generally accepted in the scientific community; 2. Whether it has been subjected to peer review and publication; 3. Whether it can be and has been tested (falsifiability); 4. Whether it has a known error rate and 5. Whether the research was conducted independent of the particular litigation or dependent on an intention to provide the proposed testimony
As reported in Wikipedia (2023), FRE Rule 702 was updated to codify and structure elements embodied in the so-called "Daubert trilogy" (i.e., Daubert and the Joiner and Carmichael cases that followed it). The amended rule is: Rule 702. Testimony by Experts: “If scientific, technical, or other specialized knowledge will assist the trier of fact to understand the evidence or to determine a fact in issue, a witness qualified as an expert by knowledge, skill, experience, training, or education, may testify thereto in the form of an opinion or otherwise, if (1) the testimony is based upon sufficient facts or data, (2) the testimony is the product of reliable principles and methods, and (3) the witness has applied the principles and methods reliably to the facts of the case.”
Rule 702 was amended again in 2011. The rule now reads: Testimony by expert witness. A witness who is qualified as an expert by knowledge, skill, experience, training, or education may testify in the form of an opinion or otherwise if: (a) The expert's scientific, technical, or other specialized knowledge will help the trier of fact to understand the evidence or to determine a fact in issue; (b) The testimony is based on sufficient facts or data; (c) The testimony is the product of reliable principles and methods; and (d) The expert has reliably applied the principles and methods to the facts of the case.
An important issue is what courts mean by the term reliability. In the courtroom, reliability takes on a scientific rather than psychometric meaning. The psychometric meaning of reliability is the degree to which a test score approximates a true score (cf. internal consistency, test-retest, split-half, alternate forms reliability) or the consistency and stability of an observation, for example, using a particular measurement tool. On the other hand, reliability in the courtroom refers to the degree to which multiple studies reach the same finding or conclusion using similar methodology and reasoning (e.g., scientific methods result in consistent findings). For instance, a pattern of EEG findings in a qEEG assessment may be reliably associated with a particular brain disorder if that association is tested in multiple scientific studies with the same result.
Courts take reliability to mean that findings of one scientific study are replicated in subsequent scientific studies (similar scientific methods in multiple studies give the same result). In matters of qEEG, psychometric reliability may be demonstrated by test-retest or split-half reliabilities showing a high correlation between data produced in the record of a single person. In court, scientific reliability may be demonstrated by finding that the association between a diagnosis such as PTSD and a particular pattern of qEEG findings occurs in more than one laboratory (cf. Greiffenstein & Kaufmann, 2018, p. 917).
After Daubert, two further cases clarified the admissibility of evidence. General Electric Co. v. Joiner (1997) strengthened the gatekeeping authority of the trial judge by specifying that extrapolation from existing data to a specific case requires more than subjective speculation (Greiffeinstein & Kaufmann, 2018). General Electric Co v. Joiner (1997) also determined that evidence should not be admitted to court if expert testimony is “connected to existing data only by the unproven assertion of the expert” because the gap between assertion and data is too large. In Kumho Tire Co. v. Carmichael (1999) found that Daubert factors apply to experts who are not necessarily scientists and that testimony can be admitted to trial not only based on scientific knowledge but also based on skill, experience, and other specialized knowledge (described by Sweet et al., 2018, p. 862). Kumho also specifically includes behavioral science and posits that the Daubert factors are not exhaustive; one or more is sufficient reason to admit or reject evidence. The Kumho court also stated that expert witnesses must use “in the courtroom the same level of intellectual rigor that characterizes the practice of an expert in the relevant field.”
Testimony must, however, be deemed admissible as evidence. Whether evidence is admissible is based on legal rules and is decided by a judge. If evidence is admitted to a legal proceeding, it may have greater or lesser weight, determined by the jury. Two sets of qEEG findings may be admissible in two different cases but assigned different relative weights by the jury depending on the particularities of the case and other evidence.
Frye and Daubert Applied to qEEG Interpretation and Use
Chartier and Evans (2023) wrote that the key element in Frye is that the science and technology from which the expert derives their opinion must be “sufficiently established to have gained general acceptance in the particular field in which it belongs” (Frye, 1923). Therefore, the field for qEEG might be “neuroscience” rather than medicine. Further, it is important to show that testimony about qEEG findings reflects valid scientific reasoning that has been appropriately applied to the facts of the case (Chartier & Evans, 2023, p. 532.)
From the point of view of qEEG experts, Chartier and Evans (2023) state that “Under the Daubert standard factors that may be considered in determining whether the methodology in question is valid are: (1) whether the theory or technique in question can be and has been tested, (2) whether it has been subjected to peer review and publication, (3) it’s known or potential error rate, (4) the existence and maintenance of standards controlling its operation, and (5) whether it has attracted widespread acceptance within a relevant scientific community.” (Chartier & Evans, 2023, p. 532.) Regarding qualification as an expert witness, Frye was superseded by Daubert and FRE 702: “if scientific, technical, or other specialized knowledge will assist the trier of fact to understand the evidence or to determine a fact in issue, a witness qualified as an expert by knowledge, skill, experience, or education, may testify in the form of an opinion or otherwise” (Chartier & Evans, 2023, pp. 532-3).
Nuwer (1997) authored a controversial position paper for the American Academy of Neurology that garnered a strong rebuttal. The position paper contended that qEEG methods posed a risk for abuse in medical-legal contexts because of false-positive results and incorrect diagnoses. The article further asserted that qEEG results could be substantially altered depending on which segments of the EEG record were selected for analysis, that test-retest reproducibility was poor, that objective safeguards to prevent errors were lacking, and that statistically significant qEEG findings might be clinically meaningless. Therefore, Nuwer concluded that qEEG was not recommended for use in civil or criminal litigation. Further, the position paper concluded that it was unacceptable for qEEG methods to be used clinically except by physicians highly skilled in EEG interpretation.
Significant rebuttals were prepared by Thatcher, Moore, John, Duffy, Hughes, and Krieger (1999) and Hoffman, Lubar, Thatcher, et al. (1999). These rebuttals showed that the AAN position paper had factual misrepresentations and omissions, relied partly on anonymous unscientific representations, and misapplied evaluative standards. Also noted was that the field of qEEG, like any area in medical science, does not produce a unanimity of unambiguous findings. As is the case in any natural science, research normally produces a range of sometimes inconsistent findings. It is unreasonable to require a standard of perfect uniformity of results for a technique to be safely applied in clinical or medical-legal settings.
Nuwer’s American Academy of Neurology (AAN) 1997 position paper that provided guidelines for qEEG was officially retired by the AAN in January 2020.
Chartier and Evans (2023) comment that qEEG findings are almost always admissible in capital cases where consideration must be given to whether the sentence of execution can be mitigated to life imprisonment because of frontal lobe dysfunction that has influenced the defendant’s character.
Thatcher, Biver, and North (2003) identify the four Daubert standards as hypothesis testing, estimates of error rates, peer-reviewed publication, and general acceptance. The Frye court required that expert witness evidence must be reliable to be admitted and defined reliability as “general acceptance.” The Daubert court continues to require general acceptance for admissibility of expert witness testimony but went further in defining general acceptance as requiring the use of scientific methods to publish findings in peer-reviewed journals.
Thatcher et al. (2003) review how qEEG methods achieve each of these four standards. Furthermore, qEEG methods are consistent with the later Supreme Court rulings on admissibility of evidence in the General Electric Co v. Joiner (1997) and Kumho Tire Co v. Carmichael (1999) cases that admit testimony based on “technical” and “other specialized” knowledge. Thatcher et al. (2003) write that the Daubert court continued to rely on “general acceptance” and defined it as occurring in a scientific community that uses the scientific method and relies on peer-reviewed publications.
The hypothesis testing criterion for admissibility under Daubert involves using the null hypothesis, which is the hypothesis of no difference between control and experimental groups or no association between variables. Such hypotheses are tested using measures with known error rates and statistical tests whose results must exceed criteria for rejecting the null hypothesis assigned before experimental investigation.
In the tradition of Karl Popper’s philosophy of science and logic that emphasizes hypothesis testing and falsifiability of the so-called null hypothesis, this involves assigning an arbitrary alpha level (e.g., .05 or 5 percent) before the experiment to define the evidentiary standard to be used.
An alpha level of .05 means that statistical tests of experimental results must reach a value with only a 5 percent chance or less of occurring by random chance. An experiment produces data subjected to statistical testing where the statistical test produces a p-value (i.e., probability that differences between groups are due to chance). The p-value is compared to the alpha level. If p is less than alpha, then the null hypothesis is rejected, allowing the experimenters to conclude that the null hypothesis of no differences between groups is false and that their experimental hypothesis of a true difference between groups fails to be disconfirmed. This 5 percent chance of incorrectly rejecting the null hypothesis is the probability of making a Type I error. A related concept is Type II error, which is the chance of failing to reject the null hypothesis when it is false.
In addition to Type I and Type II errors in experimental studies, another type of error is the measurement error of a test. Using the standard deviation of a given test’s finding, it is possible to calculate a range of numbers within which one can be 95 percent certain that the individual’s true score must occur (i.e., a confidence interval).
Peer-reviewed publication signifies that a scientist’s work is considered credible by their science community peers. The peer-reviewed publication then reflects a process of scientific exploration where the publication of a study only occurs after its experimental rigor has met demanding standards accepted by a community of scientists. Publication of the study then exposes its methods and results to scrutiny and further scientific exploration. This results in the accumulation of literature that aspires to be made up of many studies that examine a given hypothesis. That literature normally includes both confirmatory and disconfirmatory studies, which can be statistically examined in various quantitative ways (e.g., meta-analysis) to determine, for example, the overall effect size of a particular condition or experimental treatment.
General acceptance may be seen as the opinion of a particular community, for example, clinicians or scientists, about the meaning of a finding, the characteristics of a disorder, or the treatment for a specific condition. However, general acceptance can also be seen as related to the goals of meta-analysis and evidence-based medicine in which the opinions of a particular community are examined quantitatively. Evidence-based medicine has aimed to do just this and caused several conventions in health care that were generally accepted to be abandoned based on empirical investigation. For example, the general acceptance of Benjamin Spock’s recommendation of a prone sleeping position for infants to avoid choking was eventually examined with empirical evidence and rejected because prone sleeping was, in fact, associated with sudden infant death syndrome (Gilbert, Salanti, Harden, & See, 2002; Swanson, Schmitz, & Chung, 2010).
Thatcher et al. (2003) write that qEEG methods meet the Daubert standards as follows. Concerning hypothesis testing, error rate, and reliability, the authors describe the psychometric reliability of qEEG findings, for example, quantified with test-retest and split-half reliability coefficients. The authors also give the example of a cross-validation study with traumatically brain-injured (TBI) subjects to show quantitative evidence of error rates, for example, in the study’s sensitivity and specificity of classification of condition (Thatcher, North, Curtin, Walker, Biver, Gomez, & Salazar, 2001).
Thatcher et al. (2002) also give examples of how using hypothesis testing and the scientific method occurs in scientific studies that use qEEG methods, for instance, in studies of TBI subjects (Thatcher, Biver, McAlaster, & Salazar, 1998; Thatcher, Biver, Camacho, McAlaster, & Salazar, 1998). Thatcher regularly posts information on his NeuroGuide forum about the numerous peer-reviewed studies available in the National Library of Medicine that support claims of general acceptance for qEEG methods.
Moore, Shenal, Rhodes, and Harrison (1999) further describe using qEEG as part of an assessment that integrates various other data collection methods. In particular, qEEG findings can contribute to what Moore et al. (1999) describe as an a priori hypothesis testing procedure that examines the weight of combined evidence supporting or disconfirming the presence of a syndrome of interest. The strengths of qEEG assessment, according to Moore et al. (1999), are its ability to objectively test a priori predictions about brain function based on neuropsychological assessment, statistical rigor, and with some qEEG methods (cf. Bonstetter, Collura, & Cantor, 2018) the subject’s cerebral functioning during cognitive and affective challenges. qEEG findings may additionally produce hypotheses that other assessment methods have overlooked.
Admissibility of qEEG Cases
Greiffenstein and Kaufmann review several cases in which qEEG findings have been ruled inadmissible: John v. Im (2002), Nadel v. Las Vegas Metro (2001). qEEG findings as sole proof of any diagnosis have also been rejected in several criminal and civil cases: Head v. Lithonia Corp. (1989), State v. Zimmerman (1990), Ross v. Schrantz (1995), Tran v. Hilburn (1997), In re: Breast Implant Litigation (1998), Craig v. Orkin Exterminating Co. (2000), Feria v. Dynagraphics Co. (2004), LaMasa v. Bachman (2005).Thatcher (accessed 2023) presents a lengthy list of cases for which qEEG findings have been admitted as evidence in court.
Expert Witness Role
Expert witnesses provide the trier of fact with information that assists the trier of fact in making ultimate judgments about various legal issue, analysis, behavioral observations, subject and collateral informant history, review of reports, and scientific research. Expert witnesses' information may come from multiple sources, such as qEEG data and its analysis, subject, and collateral informant history. Expert witnesses may also be called to review colleagues' work, that is, without seeing the individual.Qualification as an Expert Witness
As described by Sweet et al. (2018), before evidence can be admitted in a legal matter, courts must first evaluate expert witness qualifications, the relevance of the expert’s opinions to the matter, and the reliability of bases for the evidence that will be submitted to trial (cf. FRE rules 104 and 403).Greiffenstein and Kaufmann (2018) discuss the issue of an expert’s competence to testify, citing the case of Jenkins v. U.S. (1962), which found that nonmedical professionals have a long history of being qualified to testify within their scope of knowledge. The case supports the idea that a medical degree is neither sufficient nor necessary for testimony about a person’s mental condition. Greiffenstein and Kaufmann (2018, p. 892) write that the “trial judge must determine a particular … [professional’s] qualification through a context-specific, fact-intensive exploration of [the professional’s] background, training, education, and knowledge.” The implication is that the qEEG expert must clearly demonstrate their training and qualifications related to qEEG. Board certification that requires rigorous demonstration of knowledge and skill, as shown by IQCB certification, is likely to help a judge determine whether a qEEG professional can be qualified as an expert whose opinion will have probative value in a trial or hearing.
In 2011, FRE Rule 702 was amended to make this clearer: A witness who is qualified as an expert by knowledge, skill, experience, training, or education may testify in the form of an opinion or otherwise if:
1. The expert’s scientific, technical, or other specialized knowledge will help the trier of fact to understand the evidence or to determine a fact in issue;
2. The testimony is based on sufficient facts or data;
3. The testimony is the product of reliable principles and methods, and
4. The expert has reliably applied the principles and methods to the facts of the case.
Process of Testifying
Greiffenstein and Kaufmann (2018) describe methods with which testimony by an expert under oath is given. These include written answers to questions, affidavits, discovery depositions (duces tecum subpoenas to produce materials), trial depositions (bene esse deposition to be presented later at trial), and live testimony to the trier of fact (e.g., in court). Greiffenstein and Kaufmann (2018) review elements of trial deposition, live testimony, and strategies for dealing with them (e.g., how to deal with cross-examination). Principles for testifying include detailed preparation, acknowledgment of limitations of one’s methods, and speaking in a manner intended to educate the trier of fact (e.g., judge or jury).Experts testifying about qEEG findings in court are well-advised to demonstrate how they have considered alternative explanations for their findings and the range of possible impairments that may result. In doing so, they should be prepared to comment on the sensitivity of qEEG findings and their specificity. Levels of certainty (and uncertainty) should be communicated about the association of the findings for the case and associated impairments. Opinions of these sorts should be supported by empirical research and clear neuroscientific reasoning that helps the trier of fact reach their judgment. The expert, after considering various alternative explanations for qEEG findings and alternative possible manifestations of those findings (cognitive, emotional, behavioral), provides a summary opinion of what the expert considers what what brain malady most reasonably accounts for the qEEG findings, and the manifestations of that disorder that are most reasonable to expect.
The purpose of qEEG findings in court is to provide evidence that tends to support or disconfirm the likely presence of brain anomaly. Only if the qEEG expert conducts other history taking, specialized tests, assessments, or file reviews for which they are qualified should they venture further with their testimony into the realm of the possible extent, cause, diagnosis, and effect of the brain anomaly on the behavior that is relevant to the legal matter at hand. The qEEG expert may then opine that the qEEG findings are consistent, within a given range of certainty, with brain damage related to a particular cause, for example, or to behavior of a particular type. This, however, entails understanding the sensitivity and specificity of qEEG findings for cases similar to the one for which the expert is providing testimony and alternative factors or conditions that might better account for the observed results. Testimony then describes qEEG findings as consistent (or not) with a particular brain disorder, its causes, its symptoms that may be at issue in the legal case, and the degree of certainty with which the expert holds their opinion.
When a health professional testifies about qEEG findings, their professional discipline may prepare them to gather and integrate data from other sources (e.g., personal and medical history, medical or neuropsychological test scores) with those from the qEEG. Especially in those instances, the expert may develop a logical chain of causal reasoning that allows them to opine about the likelihood that the event or exposure that is the focus of the legal case could have caused the qEEG findings. That is, qEEG findings are interpreted in the context of what is known about the association of such findings and with various etiologies and the individual’s personal and medical history (Greiffenstein & Kaufmann, 2018). For example, causal reasoning attempts to answer the question of how likely the individual’s qEEG findings are to be related to one etiology (relevant to the case) versus others and the question of how likely the qEEG findings are to be related to pre-injury and post-injury factors. Greiffenstein and Kaufmann (2018, p. 908) present several pre-accident, peri-accident, and post-accident moderator variables to consider in making a causal analysis and summarize Hill’s 1965 factors for analyzing causal statements.
As Greiffenstein and Kaufmann (2018) warn, it is important to avoid equating significantly abnormal findings with functional disability. That is, an individual’s ability or performance concerning independent activities of daily living or other tasks is only imperfectly correlated with test scores or qEEG findings. The expert’s testimony, therefore, should express caution about what can be said about the individual’s activity in normal circumstances based on the qEEG findings alone. As described above, qEEG findings provide information about the possible location and type of brain dysfunction that a defendant, plaintiff, or claimant may present. However, mere abnormality of cerebral structure or function may be irrelevant unless the abnormality is associated with abilities pertinent to the mental condition or behavior in the legal proceedings. This implies that expert testimony about qEEG findings should ideally speak to not only the degree of EEG abnormality found but also the relationship between the qEEG finding and disturbances of sensory-perceptual, cognitive, emotional, and behavioral function and how such disturbances of function are likely to appear in the environment where the plaintiff or defendant’s actions are at issue.
The expert must be able to describe the likelihood or probability of their findings and the likelihood that those findings are associated with various subjective conditions and objective behaviors. The expert witness should also discuss the typical base rates in the population of which the plaintiff/defendant/ claimant is a member for the conditions at issue, and the likelihood of alternative sources of causation. The implication of the qEEG findings for the likelihood of subjective and objective conditions in the future also merits description.
The connection between abnormal EEG or health impairment to individual experience and real-world action of a plaintiff or defendant is probabilistic and often tenuous. Therefore, testimony about qEEG findings is unlikely to be uniquely sufficient for the trier of fact to make a decision. Instead, qEEG findings may be helpful as part of a collection of convergent evidence that may support the trier of fact in making a decision with a given degree of probability depending on the civil or criminal nature of the legal action, that is, on the balance of probabilities or beyond a reasonable doubt, respectively.
Expert witnesses who present qEEG findings or are asked to conduct a qEEG for forensic matters may be requested to provide opinions regarding the existence and/or probable cause of significant findings. Doing so likely requires the integration of a considerable volume of information from diverse sources such as the qEEG itself, personal history, behavioral observation, knowledge of neuroscience and brain and behavior relationships in normal and abnormal cases, and understanding of how brain-based impairment may or may not translate into changes in functional abilities and performance. Further, knowledge about developing and using qEEG normative databases and findings with those similar and dissimilar to the plaintiff or defendant is required. Together, these sources of information, training, knowledge, and experience enable the expert witness to educate the trier of fact regarding the opinion’s degree of certainty about the existence of significant findings, their cause, and their implications. Expert witnesses are then subjected in court to direct and cross-examination, providing their opinion in a consulting role instead of the role a professional has with a patient when providing clinical and clinical assessment and treatment.
It is important to show that one’s conclusions and inferences about the data are more reasonable than other possible conclusions and inferences. If there is a significant qEEG finding, then opining that it is attributable to X must be shown to be more reasonable than attributing it to Y or Z.
It may also be important to show or consider whether findings represent a change and whether they have implications or ecological validity for ability (what the person can do as contrasted with what the person does do) and for participation in normal role activities (functional outcome) in the contexts in which they occur.
Greiffenstein and Kaufmann (2018) write that the most critical component of knowledge for an expert witness to demonstrate is the understanding of methodologies upon which their testimony is based.
Forensic vs Clinical Assessment
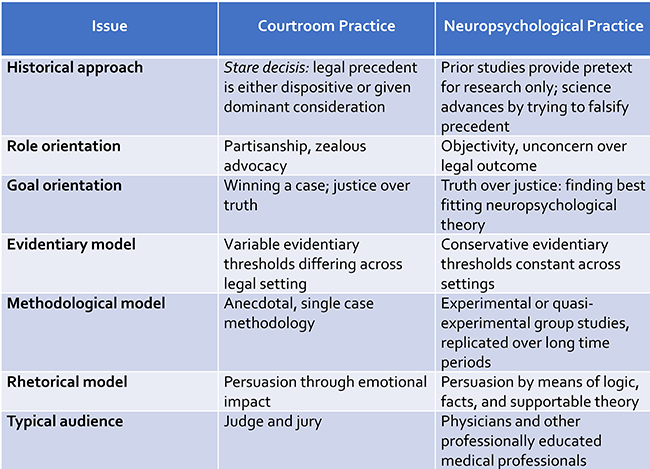
Greiffenstein and Kaufmann (2018) describe other differences between clinical and forensic assessments in neuropsychology. Some of these are presented in their table 37.1 (p. 891), which is reproduced below. It is titled “structural” conflicts because such conflicts are entailed in every case.Structural conflicts between the law and neuropsychology.
It is important to remember that even when a health professional provides clinical services to an individual who is involved in an adjudication that is potentially adversarial the services may take on a forensic nature if the professional is called to testify (Sweet, Kaufman, Ecklund-Johnson, & Malina, 2018), not as an expert witness, but as a fact witness.
Case Examples
Several case examples of qEEG in forensic settings are provided by Chartier and Evans (2023), Cantor (2009), and Yu (2020), including those of ADHD, mild traumatic brain injury, and mitigation of a sentence for murder and rape. Another is presented by Gluck (2011), who describes an example of the use of qEEG in court when the death penalty was being considered as a sentence, and where qEEG findings showed frontal lobe dysregulation consistent with the defendant’s lack of behavioral inhibition that had been a feature of his crime. The judge in this case considered the admissibility of qEEG findings, noting that it involves established (not new or novel) science, and that those findings and methods, in and of themselves, do not produce a diagnosis. The judge concluded that the qEEG data are used together with other sources of information and viewed as consistent or not with them. Of interest, the judge noted that expert agreement about qEEG need not be unanimous. The preponderance of evidence showed that disagreement was not so wide as to reject qEEG findings.Bonstetter, Collura, and Cantor (2018) describe a case involving qEEG and s-LORETA assessment with a man charged with malice and felony murder.
Fielenbach, Donkers, Spreen, Visser, and Bogaerts (2018) provide a review of studies that examine the use of neurofeedback for criminals with various psychiatric diagnoses. Mixed outcomes were found concerning changes in EEG and behavior. The edited text of Evans (2005) includes studies by several authors related to distinguishing qEEG features among criminals, subject attempts at deception, and neurofeedback with offenders. However, the literature regarding EEG abnormalities among criminals is substantial (e.g., Calzada-Reyes, Alvarez-Amador, Galan-Garcia, & Valdes-Sosa, 2021; Evans & Claycomb, 2008).
Informed Consent
Because the expert witness plays a consulting rather than treating role with the litigant, the expert witness must make their role and its limits clear to the litigant at the outset of their examination. For example, the expert should explain to the person that the “usual expectation of confidentiality does not apply, and that he or she should not provide any information to the … [expert] that he or she does not want to be revealed to all parties involved” (Sweet et al., 2018, p. 871).In cases when the expert conducts an independent medical evaluation, confidentiality is only between the expert and the referring third party, so the individual can access any report only through the referral source and not directly from the expert. Important also is ensuring that the referral question is appropriate for qEEG assessment. That is, qEEG investigation is appropriate for assessment of CNS function and structure but cannot by itself directly answer questions about cognitive, behavioral, or emotional dysfunction.
The Canadian Academy of Psychologists in Disability Assessment (CAPDA, 2000) and the American Medical Association (AMA, 2016a, 2016b) have guidelines for disability assessment. Sweet et al. (2018. p. 872) present a useful table showing details that should be reviewed with litigants or claimants at the initial meeting if not before:
1. Reasons for evaluation.
2. Referral source and relationship, if any, with the expert.
3. Description of the types of information to be collected.
4. Lack of confidentiality, making the assessment different from a normal “doctor-patient” relationship.
5. Treatment will not be offered.
6. The expert strives to maintain objectivity and does not act as a party with an interest in the outcome.
7. Importance of the examinee providing their best effort to give information and following instructions.
Patient Conditions Related to qEEG Evaluation
There are numerous potential litigant conditions for which qEEG evaluation may be useful in court. Generally, however, any cognitive, behavioral, or emotional condition that is probative or relevant to the legal action may be reasonable for making a referral for qEEG assessment. That is, a circumscribed condition such as planning ability (cognition), impulsivity (behavior), or fear (emotion) may be suitable for qEEG assessment that could then provide relevant information to the trier of fact about brain anomalies found by qEEG assessment to be related to planning, impulsivity, or fear. In other words, it is not necessary for forensic qEEG evaluation to address the full range of symptoms that comprise a clinical diagnosis. Put another way, it is most useful for the expert witness to carefully discuss with the litigator what the exact referral question is, and what information will have the most probative value. For example, an overly broad referral question such as “Is the defendant psychotic?” is not as useful as a referral question that is more focused on the crux of a defense such as “At the time of the alleged crime did the defendant have any compromise to their brain function that would be likely to impair planning and decision-making?”Limits of qEEG Interpretation
It is important to balance the potential for good and the potential for harm when testifying about qEEG in the courtroom. Caution is recommended in forensic testimony about qEEG (Coburn, Lauterbach, Boutros, Black, Arciniegas, & Coffey, 2006) because of the diversity of hardware and software used for qEEG, data processing methods, and the quality, size, and generalizability of normative databases used for comparing forensic cases. As suggested by Arciniegas (2011) and Rapp et al. (2015) the use of qEEG for TBI in forensic settings is limited by the variability of abnormalities seen, especially after mTBI, and issues of specificity and limited replication (reliability) of scientific studies on which to base testimony.Miller and Lindbergh (2018) summarize cautions for using qEEG in court. These include heterogeneity of qEEG patterns in TBI, poor specificity, insufficient replication, variability in data acquisition and analysis methods, and limited generalizability due to using only healthy database subjects. However, heterogeneous qEEG findings might be expected to some degree, given the overall heterogeneity of TBI characteristics. Furthermore, qEEG findings are very consistent with TBI findings using other imaging methods (Thatcher, Biver, Camacho, McAlaster, & Salazar, 1998; Thatcher, Biver, McAlaster, & Salazar, 1998) and successful cross-validation of mTBI case identification with discriminate function analysis have been published (Thatcher et al., 1989).
Challenges in using qEEG in court are several. The so-called “group-to-individual problem” involves the fundamental division between science, which seeks generalizable findings, and law, which seeks to reach specific judgments in individual cases. The studies on which qEEG science is based use statistical averages for groups rather than present specific information about a single person. Different courts bridge the gap inconsistently, with some allowing expert witnesses to offer conclusions for the individual case, with others restricting testimony to population-level statements while leaving it to the jury to decide the applicability of those statements to the individual case.
Confusion can also appear when testifying about significance testing, that is, the p-value, or likelihood that no difference between groups is true. Sometimes, the low p-value of .05 is misinterpreted as low confidence in any difference between groups, perhaps because experts are often asked to state their confidence level in an opinion.
Because the results of all scientific studies do not achieve uniform agreement and, in fact, may often disagree, the application of qEEG in the court may be seen as “unreliable,” in the sense that its findings are poorly replicated across studies. However, replication is not an either-or matter, and results show degrees of consistency or inconsistency. Different courts may reach different findings depending on the degree of consistency found among replications of similar studies.
The expert witness should have detailed knowledge of the specific database used for assessment, as well as its strengths and limitations. Comparison of a record to a database may well produce a statistically significant result despite the absence of any clinically significant problem. Such a challenge makes it necessary, as discussed above, to carefully correlate and synthesize multiple sources of information with statistically significant qEEG findings (e.g., direct behavioral observation, self-reported and collateral history, tests of cognitive and emotional functioning, other imaging results, reports from other expert witness and fact witnesses, basic neuroscience, behavioral neurology, real-world behavior).
A further caution is that the relationship between qEEG findings and behavior is not always clear at this stage of study. A pattern of abnormal qEEG findings might not be specific to a brain injury but related instead to a comorbid psychiatric condition or medication effect.
Ethics
Upholding the ethical standards of one’s profession is paramount. The forensic arena, however, presents additional challenges. The expert needs to maintain high ethical standards concerning an individual case. The expert must also protect the overall reputation of the qEEG field.It is important to be familiar with the ethical codes of one’s professional discipline (e.g., American Psychological Association, 2002). Codes such as those published by the American Psychological Association speak to issues such as boundaries of competence, knowledge of judicial and administrative standards, knowledge of the scientific basis for statements, comprehensive and accurate presentation of information, offering public statements, and avoidance of misleading statements by omission of crucial details.
Although attorneys advocate strongly for their clients, this contrasts with the expert’s need to be detached and objective. In some small instances, the expert must maintain their objectivity and unbiased opinion in the face of attorney pressure to provide results favoring their client.
Boundaries of competence is an important issue for the qEEG expert. This applies to qEEG findings and knowledge of the judicial rules that apply to their expert role. Different qEEG experts will have different boundaries of competence in light of their professional (e.g., neurologist or social worker).
It is also necessary to avoid speculation that exceeds what existing scientific knowledge and data allow. Said another way, existing knowledge and data will only allow opinions qualified to a particular level of certainty. Regardless of the data and the particular case, there is never absolute certainty. Verdicts by the trier of fact are made only to the standard of more likely than not or beyond a reasonable doubt.
Occasionally, one may encounter perceived unethical practices of colleagues. In those circumstances, one course of action is to wait until the legal matter has concluded before attempting to address the issue informally with the colleague. If doing so proves unsatisfactory, then a formal complaint may be made.
It is also important to note that defendants following conviction have brought actions against attorneys who have neglected to include neuroscientific evidence in their defense (Aona et al., 2019; Chartier & Evans, 2023).
Recommendations
Chartier and Evans (2023) offer several helpful recommendations for qEEG practitioners involved in forensic matters. Significantly, it is important to educate the lawyer who has engaged one’s services, as well as the defendant/plaintiff, judge, and jury, and submit peer-reviewed articles as exhibits to use. It is helpful if one can testify that one uses qEEG in one’s everyday clinical work or has published on the topic. Demystifying qEEG methods, by using concrete metaphors and using vernacular language, is also important.Chartier and Evans present a logic for the use of qEEG by those who are not physicians: they (e.g., nurses, occupational therapists, psychotherapists, psychologists) work in the domain of human behavior, assessing both normal and abnormal behavior with various techniques. qEEG methods, then, are one technique among many used in concert to understand a presenting problem, formulate a treatment plan, and perhaps make a diagnosis.
Chartier and Evans also offer an outline for sections to use in medical-legal reporting of qEEG findings (i.e., Introduction, History, Methodology, Raw data samples, Findings, Summary). It is important to interpret qEEG findings in the context of multiple sources of information, including diagnostic reports based on other methods used during the same time frame as the qEEG method. Additionally, as mentioned elsewhere, sources and methods to be considered when interpreting qEEG findings include basic neuroscience, behavioral neurology, neuropsychology, psychiatry and clinical psychology, probability and statistics, and direct behavioral observation.
qEEG data collected on the recommendation of an attorney for use in forensic matters should also be interpreted in the context of the litigant’s personal history, whether collected from the litigant themselves or from collateral informants such as family members. Additionally, academic and medical reports from earlier stages of the person’s development may be relevant.
Further Recommendations
Gluck also presents a set of excellent recommendations:1. Collect a thorough history, not only from the defendant or plaintiff, but from other sources such as collateral informants and professional reports.
2. Perform a thorough neuropsychological assessment.
3. Complete a qEEG by a professional with demonstrated training, experience, and work product involving qEEG assessment.
4. Use a database whose validity and reliability have been shown in peer-reviewed publications.
5. Educate the judge and jury about qEEG and its findings by using everyday language and metaphors.
6. Link the qEEG findings to the defendant or plaintiff’s behavior, history, and other test results.
7. Cite and explain peer-reviewed scientific articles to support interpretations.
Further recommendations for qEEG expert witness qualifications are given by Thatcher (2010). These are: 1. M.D. or doctorate in a relevant field (e.g., neuropsychology, neurology).
2. 3 years of clinical experience administering and interpreting qEEG data.
3. Board certification (e.g., International qEEG Certification Board, American Board of Electroencephalography and Clinical Neurophysiology, Biofeedback Certification International Alliance).
4. Familiarity with qEEG scientific literature.
5. Publication of scientific research related to qEEG (optional).
6. Ability to present basic information about qEEG data collection, psychometric characteristics of recordings, abnormal and normal variant EEG, etc.
7. Ability to present the original recording of EEG traces.
8. Ability to show examples of EEG traces demonstrating sections edited for analysis.
9. Ability to describe documentation for hardware and its calibration, and for software used to process data.
10. Ability to describe FDA approval status for the database used.
11. Ability to explain that qEEG findings are not a stand-alone diagnostic test.
12. Ability to state the number of database subjects used for comparison to the defendant or plaintiff.
13. Ability to provide relevant qEEG scientific publications.
14. Ability to provide relevant LORETA scientific publications.
Recommendations can also be gleaned from the text above. In addition to adhering to ethical and legal norms, detailed preparation is central. Such preparation involves thoroughly knowing the science on which testimony will be based, including its strengths and limitations. The use of peer-reviewed scientific publications with robust experimental designs and standardized measures is also more admissible and credible than so-called “junk science,” whose research relies on anecdotes, single cases, and informal measures. Clear presentation of quantitative information, consideration of alternative hypotheses, and demonstration of logical reasoning that does not go beyond available data are important. Being able to state the level of certainty about one’s opinions and the empirical basis for them is recommended. In addition to knowing the science behind one’s opinions, knowing the law regarding confidentiality and testimony is crucial.
SUMMARY
This section of qEEG Tutor has given an overview of medical-legal testimony and provides a glossary of terms below. The aim is to provide an introductory orientation to forensic use of qEEG findings so that the reader who is studying for IQCB certification can not only prepare for successful completion of the IQCB examination on Rubric IX (Clinical Practice/Forensic), but also be able to consider whether to pursue an interest in forensic applications of qEEG methods.Coverage includes a description of forensic medicine and neuroscientific evidence and a summary of research on the effects of such evidence on legal decision-making. Uses of neuroimaging in court and the value of qEEG findings in particular, are described. In addition to describing the legal settings in which qEEG testimony may occur, this section describes levels of legal authority from a U.S. perspective. The roles of the expert witness, judge, and trier of fact are outlined, along with concepts such as burden of proof, capacity, and competency.
After presenting relevant Federal Rules of Evidence, this section of qEEG Tutor describes salient U.S. Supreme Court decisions on admissibility of evidence (i.e., Frey, Daubert, Joiner, Carmichael) and how qEEG methods meet admissibility standards. qEEG cases that have been admitted to court, and those that have not are referenced. How a judge qualifies an expert witness to testify is described, and the process of testifying is outlined. Forensic and clinical assessment are contrasted. Special referral and informed consent considerations are presented, and case examples are given. Cautions, ethics, and recommendations are also summarized.
D. Correlation of qEEG Findings with Prior History and Tests
It cannot be said too strongly that qEEG findings must not be interpreted alone but must instead rely on multiple lenses that result in intersectionality of contexts rich enough to do justice to the individual whose case is before the court.
The material above, which pertains to the use of qEEG in a forensic context, underscores the practical necessity of correlating qEEG findings with other sources of information. This is particularly crucial when serving as an expert witness, testifying about a plaintiff or defendant's brain function, cognition, emotional function, or behavior. These insights are equally applicable in more typical clinical and peak performance contexts. In these settings, the use of qEEG may be aimed at formulating a presenting problem, making a diagnosis, planning a course of neurofeedback or other training/treatment, evaluating the outcome of training, or even conducting research.
The importance of integrating qEEG findings with other sources of information stems from the ultimate aims of clinicians, peak performance trainers, and scientists. That aim is to understand and influence behavior that matters in real-world contexts. Therefore, the meaning of qEEG findings becomes apparent only in the context of its relationship to other anatomical and physiological findings and psychological findings (e.g., related to cognition, emotion, and behavior). This implies measuring those other findings and correlating the qEEG findings with them. Findings also take shape because of two additional contexts: developmental and social. Therefore, the assessment of the client's personal and health history, as well as their social history, is important.
This perspective is consistent with contemporary healthcare viewpoints such as the World Health Organization's assertion of the need when understanding health and illness to integrate the tripartite framework of impairment (e.g., biological or psychological), ability (e.g., capacity to act), and participation (e.g., execution of ability in meaningful social roles).
This perspective is also consistent with the biopsychosocial framework and that of evidence-based medicine (e.g., evidence from the patient, including values and history, evidence from one's practice, research evidence, and contextual evidence related to social and material resources available). The outcome of neurofeedback training is often contingent on conditions that can only be assessed by means other than qEEG.
When formulating a presenting problem, the clinician uses more than one source of information about the client in order to have evidence that converges together to account for the problem or even for peak performance training to present a multifactorial picture of the factors that will need to be addressed, conjointly or in sequence, in order to reach the training goal. This speaks to the likelihood that no single isolated element of training or treatment will produce as robust and durable an outcome as a multi-component program of care, one important part of which may be neurofeedback.
If qEEG findings are being used as one source of information for a diagnosis, it's important to note their limitations. The sensitivity and specificity of qEEG findings for diagnoses are not high enough to make them sufficient for diagnosis on their own. Therefore, qEEG findings need to be integrated with multiple sources of information for diagnostic purposes. This is most evident when qEEG findings are integrated with neurologist or neuropsychologist reports as an adjunctive element.
When conducting a post-training evaluation of clinical or peak-performance outcomes, qEEG findings will rarely be of value by themselves. This is because the primary aim is to change the client's behavior (e.g., cognition, emotion, actions). Therefore, measures of behavior should be used in addition to qEEG findings.
Even in research settings, qEEG findings alone are infrequently the sole dependent variable of interest but are examined for their correlation with other biological or behavioral variables.
E. Appropriateness of a qEEG Referral
qEEG referrals, with their diverse purposes, underscore the crucial need to clarify the initial referral question. This step is paramount in ensuring the effectiveness and relevance of the subsequent qEEG assessment.
qEEG assessment may be appropriate for characterization of a client, diagnosis, identifying biomarkers, development of neurofeedback protocols, evaluation of outcome, and, in a scientific arena, for characterizing groups and group differences. As discussed above, qEEG is relevant for forensic applications. Usually for each of these purposes, qEEG is part of a multimethod assessment.
Although one might receive a referral for the purpose of characterizing or describing a client (e.g., “Does this client have a qEEG signature or pattern that is consistent with CNS overarousal?”), the referral source typically intends to go beyond simple description. In these cases, as noted above, it is important to clarify the referral question so as to best serve the referral source and the client.
Characterization of a client’s EEG may be requested to provide findings that bear upon a diagnosis. If the qEEG provider is a medical doctor, it is possible to entertain referrals for identifying epileptogenic activity that is relevant to the diagnosis of seizure disorder. qEEG is also a valuable tool in the differential diagnosis of dementia, monitoring neurological disorders, and assessing CNS function related to cognitive impairment in Parkinson's disease.
The effectiveness of the qEEG largely depends on the expertise of the clinicians and the quality of the laboratory performing the analysis. qEEG findings are also relevant for the diagnosis of many neuropsychiatric conditions (e.g., anxiety, PTSD, depression, ADHD, and ASD) so that the referral source may ask whether qEEG findings are consistent with any such conditions. A qEEG referral is appropriate in cases where detailed brainwave analysis can provide additional diagnostic or monitoring insights, particularly in complex neurological and psychiatric conditions.
qEEG data can also be used to identify biomarkers, not only of diagnosable conditions, but those showing likely response to treatment.
Very often, referral is made to conduct qEEG assessment to propose helpful neurofeedback training protocols.
As suggested above, qEEG methods are appropriate for monitoring neurological conditions and for providing ongoing management. Serial qEEG assessment, where a series of assessments is conducted to assess neurofeedback progress, is a common practice. This not only provides a record of progress but can also reveal a lack of progress and the need to change protocols.
In the realm of science, investigators regularly “refer,” that is, engage collaborators who conduct qEEG assessments to compare groups of subjects and changes that may result from an experimental intervention.
Additionally, in forensic settings, there are numerous potential litigant conditions for which qEEG evaluation may be useful in court. Generally, however, any cognitive, behavioral, or emotional condition that is probative or relevant to the legal action may be reasonable for making a referral for qEEG assessment. That is, a circumscribed condition such as planning ability (cognition), impulsivity (behavior), or fear (emotion) may be suitable for qEEG assessment that could then provide relevant information to the trier of fact about brain anomalies found by qEEG assessment to be related to planning, impulsivity, or fear. In other words, it is not necessary for forensic qEEG evaluation to address the full range of symptoms that comprise a clinical diagnosis.
Put another way, it is most useful for the expert witness to carefully discuss with the litigator what the exact referral question is and what information will have the most probative value. For example, an overly broad referral question such as “Is the defendant psychotic?” is not as useful as a referral question that is more focused on the crux of a defense such as “At the time of the alleged crime, did the defendant have any compromise to their brain function that would be likely to impair planning and decision-making?”
Of course, an appropriate referral may be made that requests qEEG for multiple purposes. It is important in all referrals to evaluate the referral not only in terms of whether there is scientific support for using qEEG but also in terms of one’s scope of practice. One should only accept referrals for those questions and conditions for which one has the necessary training, supervision, and professional licensure.
F. Patient Conditions Related to qEEG Evaluation
Johnstone, Gunkelman, and Lunt (2005) have proposed several EEG phenotypes that the raw EEG and qEEG can assess. Table 2 from Johnstone et al. (2005, p. 101) is reproduced below. As can be seen, these phenotypes have been clinically correlated with medication and neurofeedback protocol recommendations. Arns, Gunkelman, Breteler, and Spronk (2008) have reported that such phenotypes can be reliably assessed.
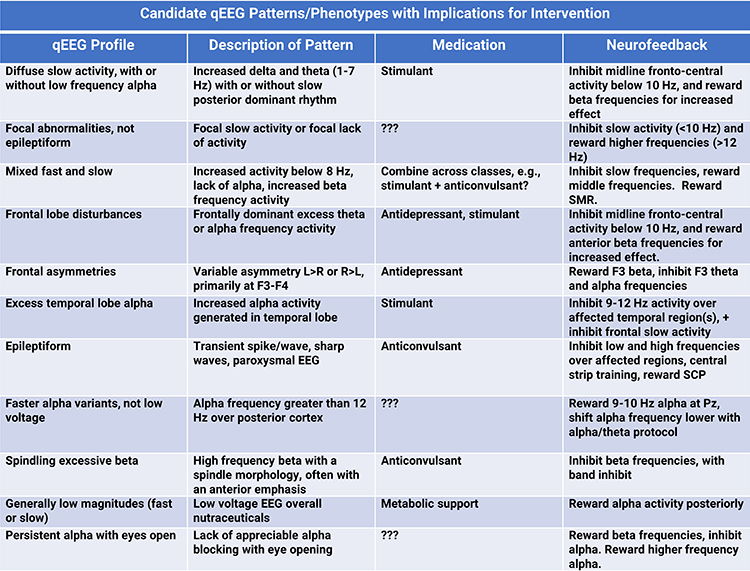
Koberda (2017) also reviews conditions for which qEEG is useful in a general neurology practice. These conditions include traumatic brain injury, cerebrovascular accident, pain and headache, depression and anxiety, cognitive dysfunction, Alzheimer's disease, autism spectrum disorder, ADHD, seizures, and epilepsy. Kropotov (2016) reviews neuromarkers, including qEEG findings, that are helpful for the early identification, prevention, and personalized treatment of several mental disorders, such as ADHD and schizophrenia.
Diagnosis and Management
The qEEG has proved valuable in the diagnosis and management of ADHD, dementia, neurological disorders, Parkinson's Disease, and refractory patients. The qEEG is a valuable tool in the differential diagnosis of dementia, monitoring neurological disorders, and assessing cognitive impairment in Parkinson's disease. The effectiveness of the qEEG largely depends on the expertise of the clinicians and the quality of the laboratory performing the analysis. Therefore, a qEEG referral is appropriate in cases where detailed brainwave analysis can provide additional diagnostic or monitoring insights, particularly in complex neurological and psychiatric conditions.Attention Deficit Hyperactivity Disorder (ADHD)
Evidence from multiple studies supports the appropriateness of qEEG as an auxiliary tool in the diagnosis and management of ADHD. It provides objective data that can complement traditional diagnostic methods, help identify ADHD subtypes, and guide treatment planning.Research has identified distinct qEEG subtypes within the ADHD population, indicating that children with ADHD do not constitute a neurophysiologically homogenous group. These subtypes are characterized by different patterns of brain wave activity, such as elevated delta power or increased alpha power, which can aid in more accurate diagnosis and understanding of ADHD (Byeon et al., 2020).
A systematic review highlighted that qEEG parameters could help characterize ADHD subtypes, contributing to personalized and more effective treatments (Galiana-Simal et al., 2020). qEEG data have been shown to correlate with symptom severity in ADHD patients. For instance, theta-band power was positively correlated with inattention scores and reaction times, while gamma-band power was correlated with auditory continuous performance test result (Roh et al., 2015).
Differential Diagnosis of Dementia
The qEEG is useful for differentiating between various forms of dementia, such as Alzheimer's disease, Lewy body dementia, Parkinson's disease dementia, frontotemporal dementia, and vascular dementia. Specific qEEG patterns, like EEG slowing and coherence changes, help in distinguishing these conditions (Poa et al., 2020).Diagnosis and Monitoring of Neurological Disorders
The qEEG is valuable in diagnosing and monitoring neurological disorders, including epilepsy, vascular diseases, dementia, and encephalopathy. It provides detailed brain wave data that can complement traditional diagnostic methods and assessments (Kopańska et al., 2022; Valdés et al., 2005).Assessment of Cognitive Impairment in Parkinson's Disease
qEEG measures, particularly those reflecting EEG slowing (e.g., decreased dominant frequency and increased theta power), correlate with cognitive impairment in Parkinson's disease and can predict future cognitive deterioration (Geraedts et al., 2018).Refractory Patients
Swatzyna et al. (2016) proposed that isolated epileptiform discharges (IEDs) may be a transdiagnostic biomarker for refractory cases without seizures. Of 76 refractory patients presenting with IEDs and treated with anticonvulsants, 65 (86%) improved, 6 (8%) were unchanged, and 5 (7%) deteriorated.A systematic review by Swatzyna et al. (2022) concluded that IEDs were highly prevalent in children and adolescents without seizures diagnosed with ADHD (>25%) and Autism Spectrum Disorder (>59%). The prevalence was low (3%) in depression.
General Clinical Utility
The qEEG is beneficial for detecting organic brain dysfunctions, categorizing clinical conditions, and localizing epileptic sources. However, its effectiveness depends on the competency of the clinicians and the quality of the laboratory performing the analysis (Duffy et al., 1994).G. History and Prior Clinical and Laboratory Reports Review
Intake assessment is the foundation for diagnosing and selecting evidence-based interventions to treat symptoms or improve performance. Assessment should be multimethod, evidence-based, and culturally competent.
Multimethod assessment means using several assessment tools since no single tool can evaluate all relevant personality and behavioral domains. Depending on provider scope of practice and client presenting concerns, an intake may include inventories, behavioral assessment, and file review (Pomeranz, 2020).
Evidence-based assessment reflects the movement toward evidence-based treatments. Professionals should select measures that work and are psychometrically validated (e.g., reliability, validity, and clinical value). For example, the Beck Depression Inventory-II is widely used to help diagnose adult depression (Pomeranz, 2020).
Culturally competent assessment is sensitive to a culture's definition of normality and abnormality. Providers understand the relevant cultural norms of the populations they serve (Pomeranz, 2020). They avoid overpathologizing and labeling culturally normal behavior as abnormal, by viewing behaviors, cognitions, and feelings using the lens of the client's culture [rather than the provider's culture]. Dana (2005) has described ignorance or insensitivity to cultural norms as cultural malpractice.
Intake assessment has several purposes and methods. The use of these methods produces various quantitative and qualitative types of information. After collecting intake information, the practitioner integrates it with EEG findings and their clinical experience and knowledge of the science on which neurofeedback is based. The practitioner then shares a holistic summary with the client to arrive at a mutually agreed-upon common understanding of the presenting problem, a goal, and treatment options to decide whether to embark on a particular course of NFB training. Graphic © Motortion Films/Shutterstock.com.

Intake Assessment
Purposes of Intake Assessment
The general purposes of intake assessment include gathering information, sharing information, and decision-making. In parallel to these, an essential purpose is to build a trusting working relationship that inspires confidence that neurofeedback will help. The results of the intake assessment describe the problem qualitatively and quantitatively and provide the baseline against which progress is measured. The information from intake contributes to constructing a formulation of the problem, that is, understanding why the problem occurs and what will alleviate it. This formulation sets the stage for planning neurofeedback training and helps the client give informed consent. In some clinical practice situations, another purpose may be to diagnose.Optimum Performance Assessment
Some practitioners focus their neurofeedback practice and biofeedback on what is variously known as peak performance, optimum performance, or simply performance training. Individuals who present for such training do not generally perceive themselves as having a "presenting problem" but primarily want to improve their performance in a sport, a musical career, academic achievement, or other endeavors. For such clients, assessment goals are quite similar to that of the clinical client. Identifying levels of function and differences from typical and other measures can be beneficial in guiding optimum performance training. The ultimate goal is performance enhancement. The desired outcomes are often measured by indicators specific to the client’s interests, such as improved scores, better ratings, improved musical opportunities, improved academic results, and the like.When working with optimum performance clients, the assessment may reveal a clinical issue, and sharing this information with the client can be a delicate task. Also, practitioners who are not licensed or registered health professionals may not even recognize such issues and may train the client in ways that may exacerbate such findings. Thus, it is vital for practitioners working with optimum performance clients to use comprehensive assessment techniques described in this section to ensure a thorough understanding of the client is obtained to avoid adverse outcomes.
Intake Assessment Methods
A neurofeedback practitioner's methods during their intake assessment are guided by the nature of the presenting problem, goal, practitioner skill set, client wishes, and tools available. Some of the methods outlined below (e.g., questionnaires and rating scales) may be carried out before first meeting the client, whereas others (e.g., tests) may occur during or after an initial appointment.Preliminary Steps
After the client or referral source contacts the practitioner to request neurofeedback, the practitioner may use that initial contact to collect basic background information, either by phone or by sending a questionnaire. Suppose a background questionnaire is sent to the client. In that case, it may be accompanied by standardized or non-standardized rating scales or other questionnaires that the client is instructed to complete and bring with them to their first face-to-face meeting. Alternatively, background forms, questionnaires, and rating scales may be administered at the practitioner’s office before the intake interview. Some questionnaires and tests may even be completed online prior to the first face-to-face meeting. If the client is a child, then questionnaires and rating scales may be sent to the parent or some other significant person in the client’s life, such as a teacher. Consent forms can also be sent in advance.Introduction and Consent
For the first face-to-face meeting, the provider needs to introduce themself and outline the methods involved in the intake assessment. This enables the client to participate to the best of their ability. An essential part of intake assessment occurs at the outset with a review of confidentiality and the limits of confidentiality before verifying that the client then wants to proceed. Consent should be documented.Throughout the intake assessment, the provider should use active listening skills and other supportive communication skills to build a working relationship with the client (Silverman et al., 2013). The use of these skills fosters trust and credibility and puts the client at ease to provide the best possible information to the practitioner.
If identifying information details are not fully collected before the intake interview, the practitioner can ask the client directly for particulars such as name, birthdate, address, phone number, information related to billing and whom to contact in the case of an emergency.
Problem Description
Following this opening introduction, information needs to be gathered about the client’s presenting problem and goal (Schwartz, 2016). This may begin with a simple open-ended question, allowing the client time to respond. A great deal can be learned in these first few minutes of an interview by listening to clients present their concerns and goals unimpeded and in their own words. The practitioner can then better follow up with specific questions to understand the problem more thoroughly.Inquiry about the details of the presenting problem helps to construct a description or definition of the client’s primary concern. The problem may be an excess or a deficit and may relate mainly to the client’s emotional, thinking, or somatic functioning. The problem definition may include information related to frequency, intensity, and duration of occasions when the problem occurs.
Context matters so that motivational conditions, antecedents, and consequences of the behavior may be helpful to describe. When the problem first had its onset and surrounding circumstances may be relevant to the assessment. How the symptom has waxed and waned over time and factors that worsen or relieve it can be valuable pieces of information. What the client and others have attempted insofar as changing the problem is also essential, and whether the client is receiving any ongoing treatment. How the issue affects or limits the client helps to illustrate the severity of the concern.
The provider and client use this information to define a goal for training, for example, to decrease a problem that represents an excess of some sort or to increase function that is deficient in some respect. Of course, the results of EEG assessment are part of goal-setting.
Personal and Family History
Information about the larger context of the problem is essential (Stucky & Bush, 2017). Categories of such information are referred to as personal and family history. The client’s personal history includes medication, drug and alcohol use, diet and exercise, sleep, medical issues, psychiatric problems, family and social relationships, education, work experiences, legal matters, and military service. In several of these categories, it is helpful to inquire about treatment, training, and unique accommodations that the client may have had. The client’s typical level of function is beneficial to elicit. This may be done for personal care, completion of domestic chores, socialization, community access, education or work, and leisure and recreation.Family history contains relevant information about parents, siblings, and possibly other family members. Although topics noted for personal history can serve as areas of inquiry about family members, it is usually the case that collection of family history information is more focused and limited to items that are particularly relevant to the client’s presenting problem and goals (e.g., medical and psychiatric concerns).
Diagnostic Interviewing
For some registered/licensed health professionals, the intake information may contribute to making a diagnosis. Several semi-structured interview formats have been developed to elicit information for making a psychiatric differential diagnosis. Medical practitioners may also make a diagnosis based on an interview, physical examination, and test findings.Barriers, Strengths, and Client Perspective
In addition to describing the problem and its course and outlining likely contributing factors, the intake interview also examines possible personal, social, and material resources available to aid in problem resolution. These may include, for example, motivation, encouraging family members, and access to transportation or the internet. Barriers may similarly be personal, social, or material. Additionally, the client’s view of the causes of the problem and what it will take to remedy it are valuable points of inquiry.Behavioral Observation and Mental Status Examination
The client’s way of moving and speaking during the intake interview can be very informative in arriving at a description of the problem and goal and understanding the client.In some clinical situations, the practitioners may administer more formal questions to understand the client’s emotional and cognitive condition. A mental status exam (Sadock et al., 2017) provides a format for observation and briefly assessing mental functioning. Topics include speech, emotion and affect, thought content and form, perceptual disturbances, cognition, reasoning, insight, and judgment.
Collateral Interview
Especially with clients who may be unable to provide reliable information, an interview with a close relative or someone with significant direct experience with the client is beneficial. This information may fill in gaps left from the client interview and add new information. Inconsistencies between the client and collateral information may also suggest potential client deficits.Reports
Several types of reports may be relevant to intake assessment. These include medical and psychiatric reports and academic and vocational information. If the client has been referred by another professional, a report from that professional can be illuminating. Although such a report may be written, a phone conversation with a referral source can be very informative. Such a conversation can help to clarify the reason for referral, attainable goals, and likely predisposing, precipitating, and perpetuating causes for the problem. The client should be asked for their consent to request reports that are likely to be helpful.Questionnaires and Rating Scales
Questionnaires often consist of checklists and places for clients to respond in their own words. This allows the client to provide basic background information, problem description, and personal history. Items may be open-ended and qualitative (e.g., describe your concern), closed-ended (e.g., have you ever had a seizure), or multiple-choice (e.g., check each type of caffeinated beverage you drink).Rating scales help to quantify a problem (Baer & Blais, 2010). They may be standardized and have norms that compare the client’s results with those of groups matched to the client, for example, based on age or education. Alternatively, they may be constructed with items the provider has developed for use in their specific setting and may or may not have norms developed in the practitioner’s office.
Both questionnaires and rating scales can collect information about cognitive, emotional, behavioral, and physical symptoms or problems (Psychology Tools, n.d.). They can also gather information about the functional consequences of symptoms: the effect that they have on practical, real-world ability and social adjustment (Űstűn et al., 2010).
Information from questionnaires helps describe the presenting problem in qualitative terms and gives the provider insight into how the client sees the problem. Rating scales, together with EEG results, provide quantification of the problem and serve as a baseline for recognizing progress or the lack of progress once training has begun.
As noted above, questionnaires and rating scales can be sent to the client in advance of the intake interview or completed immediately before or after the interview. Collecting information by questionnaire can make the intake interview much more efficient and help focus the interview on the most salient aspects of the client’s concerns.
Whereas some questionnaires and rating scales are proprietary, others are available in the public domain. Informant versions of some questionnaires are also available.
Cognitive Tests
Not only in research settings but frequently in clinics, practitioners will often administer tests of thinking and cognition (Lezak et al., 2012). Depending on the goals of neurofeedback for a particular client, domains assessed may include one or more of the following: attention, memory, language, visual-spatial perception and construction, and executive functioning. Intellectual functioning, academic performance, sensorimotor ability, and effort/performance validity may also be assessed. For example, deficient attention may be why the client requested neurofeedback. A continuous performance test such as the Conners Continuous Performance Test (2014) may be used to assess sustained attention and distractibility. Graphic © Pearson.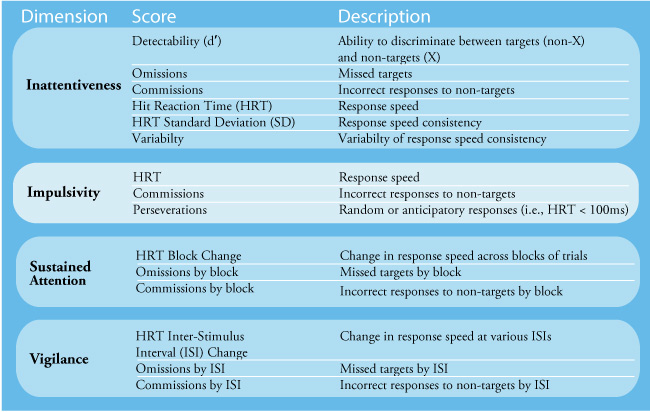
Or, improved academic performance may be the client’s goal, with the practitioner using an educational screening instrument such as the Wide Range Achievement Test (Wilkinson & Robertson, 2017). Graphic © Pearson.
Alternatively, a measure of intelligence (e.g., Wechsler Adult Intelligence Scale-IV; Wechsler, 2008) or collection of executive function or cognitive self-regulation measures may be of interest (e.g., Delis-Kaplan Executive Function System; Delis et al., 2001). Cognitive test batteries have several tests that assess representative domains of cognition and may include, for example, measures of aspects of attention, memory, and executive function (e.g., CNS Vital Signs; Gaultieri & Johnson, 2006). Graphic © Pearson.

Tests should be selected critically, considering standardization methods, normative groups, reliability, and validity. Many tests are available only to professionally qualified health practitioners, while many other tests can be purchased with fewer requirements. While many tests use paper and pencil or objects to manipulate, additional tests are administered by computer.
Those tests that use paper and pencil, or manipulable objects, usually require administration by a well-trained individual. However, those tests administered by computer reduce the cost of clinician time, both for administration and scoring. Nevertheless, a practitioner should interpret results with appropriate professional background for the results to have validity and value for the client.
Psychophysiological Assessment
Some practitioners integrate neurofeedback with other treatment modalities they are trained to offer. These may include counseling or psychotherapy, medication management, audiovisual entrainment, brain stimulation, or peripheral biofeedback. For the latter, psychophysiological assessment can help identify which physical system to treat and provides a baseline for judging progress (Khazan, 2013; Peper et al., 2008).The quantitative data collected during intake assessment, whether from rating scales, questionnaires, cognitive tests, IQ and academic measures, or psychophysiological analysis can serve as an important baseline reference point for evaluation the effects of training and for decision-making during the course of neurofeedback.
EEG Assessment for Neurofeedback
Depending on the presenting problem and goal, and practitioner training, initial EEG assessment may be more or less elaborate. The complexity of the initial evaluation also relates to the number of electrode sites used, which, in typical neurofeedback practices, ranges from 1 to 19.
In addition to examining the analog waveform of the EEG signal, several variables can be evaluated quantitatively. Data from single sites may be represented by absolute or standardized (i.e., z-scores) values of amplitude or power in single-hertz bins or frequency bands that span a range of hertz values. Power values may also be given in ratios that compare bands.
Dr. Ronald Swatzyna has generously permitted the authors to share the Houston Neuroscience Brain Center's client orientation video.